The post Treatment challenges in MIBC: ctDNA, EV-P cost and access appeared first on EMUC25.
]]>For ctDNA-positive patients, adjuvant immunotherapy can be offered, with demonstrated treatment efficacy in a predominantly clinically high-risk population (IMvigor011), and a 50% ctDNA clearance in both low- and high-risk groups (TOMBOLA).
Prof. Dyrskjøt: “Overall, ctDNA-based molecular stratification outperforms clinical and histopathological risk assessment in identifying patients who benefit from adjuvant treatment, as shown in both IMvigor011 and TOMBOLA.”
In regard to the requirements for implementing ctDNA-guided care, Prof. Dyrskjøt stated that “Sensitive tumour-informed tests are required. Continued ctDNA analysis is needed, a single test post-RC is not enough, and assay availability and fast turnabout time are essential. We need to generate knowledge on how to bridge and use ctDNA in the peri-operative setting (NIAGARA, KEYNOTE-905/EV303, etc.).”
On his overall view on ctDNA use, he concluded, “Yes, it can be used for guiding adjuvant immunotherapy. But for guiding pre-cystectomy treatment – no, not yet; we need more studies first.”
Following this was a presentation on ‘Treating metastatic bladder cancer when money is an issue’, by Dr. Jorge Estaban Villarrubia (ES). “Back in October 2023, we were all excited about the enfortumab -vedotin + prembrolizunam (EV-P) data presented, and then the 2024 guidelines were updated and the EMA granted approval for the new combination.”
But according to Dr. Estaban Villarrubia, it is important to note that although the survival rates of this combination therapy are impressive, its high-cost limits broader use in many public health settings. In addition, some countries (including Spain) are still awaiting approval of EV-P, and there is also the issue of access to NGS (next-generation sequencing) which is not readily available in all hospitals.
“As oncologists, we must ask some important questions when we can’t get the best systemic therapy. What are the next best options for maximising treatment benefit, without increasing toxicity? Is there a role for radical treatment options?”
He reviewed treatments such as chemotherapy (cisplatin), split dose cisplatin for cisplatin-ineligible symptomatic patients, as well as strategies supported by evidence to reduce the number of cycles in order to minimise toxicity.
In his take-home messages, he concluded, “When money is an issue, we still have therapeutic options with proven efficacy. Collaboration between institutions is key to providing access to precision medicine, clinical trials and best available care. Multidisciplinary management of the patient leads to better outcomes, not only in survival, but quality of life, too. We must not forget that palliation is an important target of our treatment.”
For more information, you can (re)watch the presentations via the EMUC25 Resource Centre.
The post Treatment challenges in MIBC: ctDNA, EV-P cost and access appeared first on EMUC25.
]]>The post Personalised approaches to treating GU cancers appeared first on EMUC25.
]]>Prof. Lars Dyrskjøt (DK) opened the session with his presentation “Circulating tumour DNA for decision-making in high-risk and metastatic bladder cancer.” He first gave his audience a quick refresher on ctDNA. “Mutated DNA from cancer cells is shredded into circulation. This is named ctDNA, and we can use it as a very sensitive and specific biomarker for tumour burden and metastatic spread.”
“ctDNA has the potential to be used throughout the disease course in patients with cancer,” Prof. Dyrskjøt stated. “We can use it for risk assessment before treatment and cystectomy, as a profiling tool for prognostication, for early diagnosis of minimal residual disease after radical cystectomy, and to monitor treatment response during, for instance, chemo- and immunotherapy.”
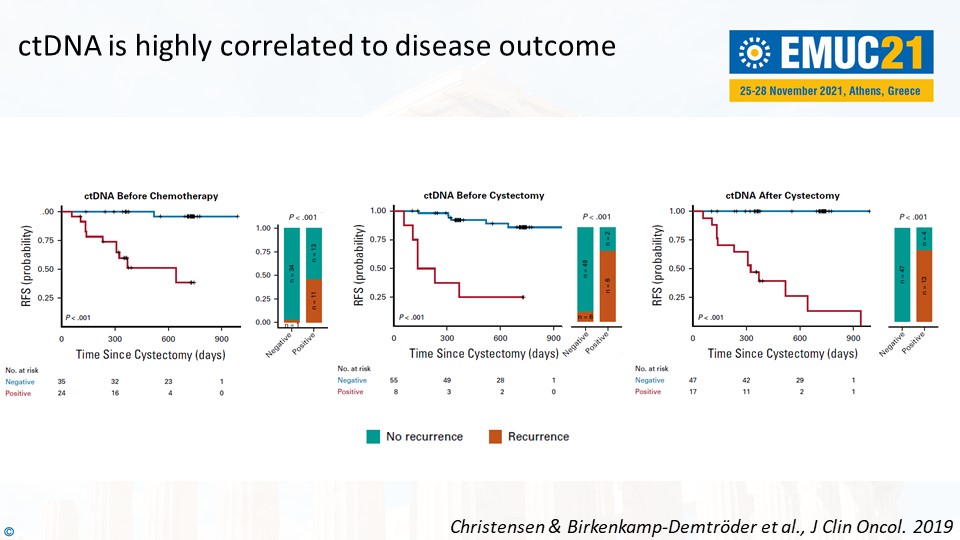
Prof. Dyrskjøt mentioned the results from a prospective study he worked on to support these statements. For instance, ctDNA-negative patients were associated with good outcomes – and the other way around. “It is a highly prognostic factor to be ctDNA-positive. ctDNA is highly correlated to disease outcome,” he said, referring to the slide below.
Prof. Dyrskjøt concluded, “What we need to demonstrate now is the clinical impact of ctDNA-based guidance. Can it improve the overall survival? Can it improve the quality of life? Can we reduce costs?”
Practical tips on genetic testing in prostate cancer
In the following presentation, Dr. Elena Castro (ES) gave practical tips on genetic testing in prostate cancer to the attending delegates. “We should consider assessing the HR status early, because it may take some time to retrieve blocks or to consider a re-biopsy. It’s good to know that the BRCA1/2 mutations rarely change status over time. Poly (ADP-ribose) polymerase inhibitors are currently approved after progression to androgen receptor signalling inhibitors (ARSis).”
“Finally, we should offer germline testing to all patients with metastatic prostate cancer. Somatic tests are not validated for germline assessment. We shouldn’t forget to exclude the potential germline origin of the mutations in the cancer-related genes from tumour analyses.”
The other two lectures in Plenary Session 8 were presented by Dr. Maria Rosaria Raspollini (IT) and Prof. Francesco Ceci (IT). (Re)watch all presentations of Plenary Session 8 as webcasts in the EMUC21 Resource Centre. EMUC21 delegates can access all scientific content here. All presentations, full-text abstracts, and (e-)posters are easily accessible in the Resource Centre.
The post Personalised approaches to treating GU cancers appeared first on EMUC25.
]]>The post EMUC18 addresses current dilemmas in mPCa treatment appeared first on EMUC25.
]]>“There is a strong unmet need for prognostic and predictive biomarkers to guide treatment of mPCa. We have this increasingly congested therapeutic landscape and a shift in consensus on when and how to best use these therapies,” said Assoc. Prof. Alexander Wyatt (CA). “How do we determine the optimal therapy and sequence of therapies for patients? Can tumour molecular subtype (genomics) help guide these decisions?”
In his lecture “Cell free DNA in blood: The best source for response prediction?”, he stated that one of the strengths of plasma cell-free DNA analysis is that all patients are eligible for blood-drawing; while with metastatic tissue biopsy, some patients may ineligible e.g. patients with aggressive diseases that have rapid deterioration.
According to Prof. Wyatt, serial sampling is more advantageous in a liquid biopsy setting as it is less complex. However, ctDNA does not provide information in all patients. “Another potential benefit of ctDNA is that it captures information from multiple metastatic sites while tissue biopsy which informs from a single metastatic lesion only. On the other hand, if a tissue biopsy can provide a very high-resolution of that single lesion, it will allow us to understand what is going on in a single metastatic site as ctDNA homogenizes heterogeneity. ”
Oligometastasis
In his lecture “Why do some patients only get oligo-metastatic disease?”, Dr. Ganesh Palapattu (US) emphasised treating the patients, not the diseases. “Not all prostate cancer patients are the same. Now we are treating fewer low-risk patients, and that is a good thing, and more high-risk cases. We’ve learned that there is a significant benefit for risk-based treatment allocation. We can’t treat all patients the same way. The diseases don’t behave in the same way.”
According to Dr. Palapattu, the term “oligometastasis” was originally coined by Dr. Samuel Hellman and Dr. Ralph Weichselbaum, and defined it as “An intermediate state of cancer spread between localized disease and widespread metastases”.
He stated, “If we’re going to treat oligometastasis effectively, we need to think about three main things: treat the primary because it is the important source of cancer cells; treat the metastasis that we can see; and treat the ones you can’t.”
For more information and to access webcasts and abstracts, check out the EMUC18 Resource Centre.
The post EMUC18 addresses current dilemmas in mPCa treatment appeared first on EMUC25.
]]>